
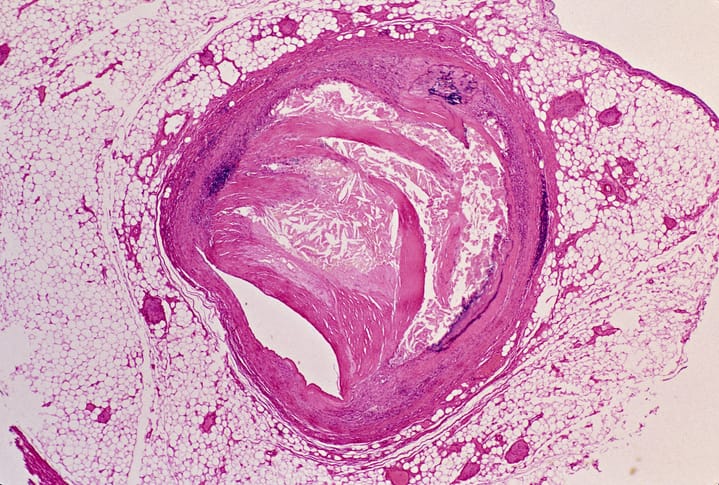
Destabilizing TTR variants associated with increased mortality in ATTR-CM
Patients with ATTR-CM and destabilizing TTR variants appear to have higher all-cause mortality than patients with stable variants.
Patients with ATTR-CM and destabilizing TTR variants appear to have higher all-cause mortality than patients with stable variants.
Older patients faced a higher prevalence of coexisting cardiac amyloidosis, including ATTR-CM, and coronary artery disease.

Patients with ATTR-CM on vutrisiran had a reduced risk of death and cardiovascular events.

Sodium-glucose cotransporter 2 inhibitors (SGLT2i) could have a therapeutic benefit for patients with ATTR-CM.

Trimetazidine did not improve heart function or exercise capacity in patients with wild-type transthyretin cardiac amyloidosis.
Despite relatively recent diagnosis (four months), most patients had advanced transthyretin amyloid cardiomyopathy (ATTR-CM).

Ventilation abnormalities appeared to play a more important role in ATTR-CM-associated shortness of breath than cardiac output abnormalities.

If approved, vutrisiran would become the first U.S. treatment to treat both polyneuropathy and cardiomyopathy linked to ATTR.

Nine years of treatment with tafamidis prevented hospitalizations for heart failure in two patients with ATTR-CM.

ATTR-CM is thought to affect mainly men. But recent studies suggest that more women could have the disease than earlier thought.
